Hip Impingement: The Hidden Back Pain Trigger You’ve Never Linked to Your Aches
Hip Impingement: The Hidden Back Pain Trigger You’ve Never Linked to Your Aches
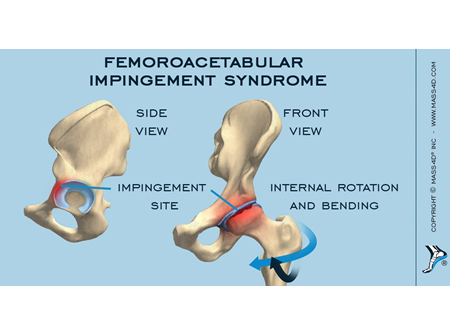
Beneath the surface of everyday back discomfort lies a lesser-known but increasingly recognized cause: hip impingement—a subtle misalignment that restricts movement, generates chronic strain, and drives back pain in ways most overlook. For years, suffering from lower back stiffness has been attributed to poor posture, heavy lifting, or aging; yet recent clinical insights reveal that the hip joint itself may be the unexpected source of irritation. Hip impingement—often described as a “pinching” or “crowding” of the hip joint—happens when the femur (thigh bone) impacts the pelvis or surrounding bony structures, particularly during motion.
Unlike common causes such as disc degeneration or muscle strain, this condition disrupts biomechanics in a way that rarely registers on standard imaging, yet profoundly affects functional movement. As Dr. Elena Marquez, an orthopedic specialist at the Institute for Musculoskeletal Health, explains, “The hip isn’t just a ball-and-socket joint—it’s a dynamic system.
When movement becomes restricted, compensations ripple through the spine, rearranging forces that trigger pain far beyond the joint zone.” The mechanics of impingement involve a clash of anatomy designed not for conflict. The hip’s acetabulum (socket) and femoral head are meant to glide smoothly. When misalignment occurs—often due to structural differences, uneven muscle activation, or repetitive motions—the femoral head may collide with the pickup edge of the pelvis, known as the acetabular rim or the “coxofemoral impingement zone.” This friction generates microtrauma, inflammation, and scar tissue formation, all signaling pain.
Unlike acute injuries, this process unfolds gradually, with symptoms worsening over months or years until patients experience persistent dull aches, stiffness, or sharp discomfort during activities like walking, climbing stairs, or even sitting.
One of the most insidious aspects of hip impingement is its mimicry of other back ailments. Stiffness and localized tenderness are common signs shared by disc herniations, facet joint osteoarthritis, and spinal stenosis.
However, unlike those conditions that target spinal structures directly, hip impingement imposes mechanical stress from beneath. This means a patient with hip-driven pain may be misdiagnosed with a purely spinal issue—leading to treatments that address symptoms but not the root cause. “Many patients undergo spinal injections or decompression only to find relief is temporary—because the real issue isn’t the spine itself, but the bony architecture deep in the hip neighborhood,”
Who is most vulnerable? Research identifies a profile shaped by both structural and behavioral factors.
Individuals with congenital differences—such as femoral anteversion (a inward tilt of the femoral head)—face higher risk. Athletes who engage in repetitive hip-driven motions—runners, cyclists, or players in sprinting sports—often exhibit early signs due to overuse and repetitive strain. Even sedentary lifestyles contribute: prolonged sitting compresses the hip joint, encourages tight hip flexors, and encourages pelvic misalignment, all amplifying impingement potential. “It’s not just athletes,” says Marquez.
“Modern sedentary habits create a perfect storm—tight connective tissues, weak glutes, and altered gait patterns all converge to pinch the joint without a single acute injury.”
Anatomical Triggers and Biomechanical Breakdown
The most common form, impingement type I (cam lesion), arises when the femoral neck protrudes farther into the socket than normal, diminishing space for movement. Type II impingement, or pincer lesion, occurs when the pelvis itself—via overcoverage of the acetabulum—impinges on the femoral head. In some cases, mixed or type III presentations combine both structural and soft tissue contributions, increasing pain severity.Clinicians rely on a targeted diagnostic approach: - **Physical exams** assess joint range of motion, pin-down signs, and muscle tightness around the hip - **Imaging modalities** include MRI for soft tissue evaluation, and CT scans specifically highlighting bony abnormalities - **Movement patterns**—such as hip agility during a Thomas test or left/right pelvic droop—reveal asymmetries feeding impingement Everyday motions that once seemed harmless can now be seen through a new lens. The repetitive flexion of a plasterer’s bent waist, a teacher’s prolonged standing, or even a runner’s anatomically pronounced hip rotation may escalate impingement without conscious pain during the act.
Treatment strategies diverge from numbing agents toward restoring functional alignment and restoring mobility.
Conservative management—physical therapy targeting hip abductors, extensors, and core stabilizers—often yields measurable improvement. Targeted stretches ease tight iliotibial bands and gluteals, while strengthening weak muscles corrects pelvic sway. Over time, this reduces joint compression and redistributes forces more evenly across the spine and hip complex. “True healing comes from retraining movement,”
“When we fix the hip, the back often follows,” explains Dr.Marquez. “It’s a network effect—aligning one joint reverberates through the kinetic chain. Minimally invasive options remain reserved for persistent cases, including arthroscopic surgery to reshape the acetabulum or excise impinging bone—procedures offering relief but reserved after exhaustive nonoperative intervention. Preventative measures gain urgency in light of rising hip impingement cases tied to lifestyle patterns. Simple adjustments—ergonomic workstations, mindful movement during daily chores, regular hip mobility drills—can disrupt the cascade from misalignment to chronic pain. In essence, hip impingement reveals that back pain isn’t always a spinal story.
It’s a movement disorder rooted in biomechanics, where the hip joint—often overlooked—holds lessons critical to long-term relief.
The evidence is clear: chronic back pain may sometimes spring not from the spine, but from beneath it—where the hip’s hidden jiggle damages motion from within. Recognizing hip impingement as a primary driver empowers individuals and clinicians alike to shift from reactive care to proactive correction, restoring function and ending the cycle of silent pain.


Related Post

Exploring The World of 5Starsstocks.com Healthcare: A Deep Dive into a Rising Force in Medical Innovation

Mastering the Furnace Stardew: The Complete Guide to Powering Your Homestead

The Los Angeles Center for Law and Justice: Championing Equity in a Complex Urban Landscape

Who Owns Dodge? The Auto Giant Behind America’s Iconic Muscle Car Brand